Class 11
Created by Titas Mallick
Biology Teacher • M.Sc. Botany • B.Ed. • CTET (CBSE) • CISCE Examiner
Created by Titas Mallick
Biology Teacher • M.Sc. Botany • B.Ed. • CTET (CBSE) • CISCE Examiner
Online
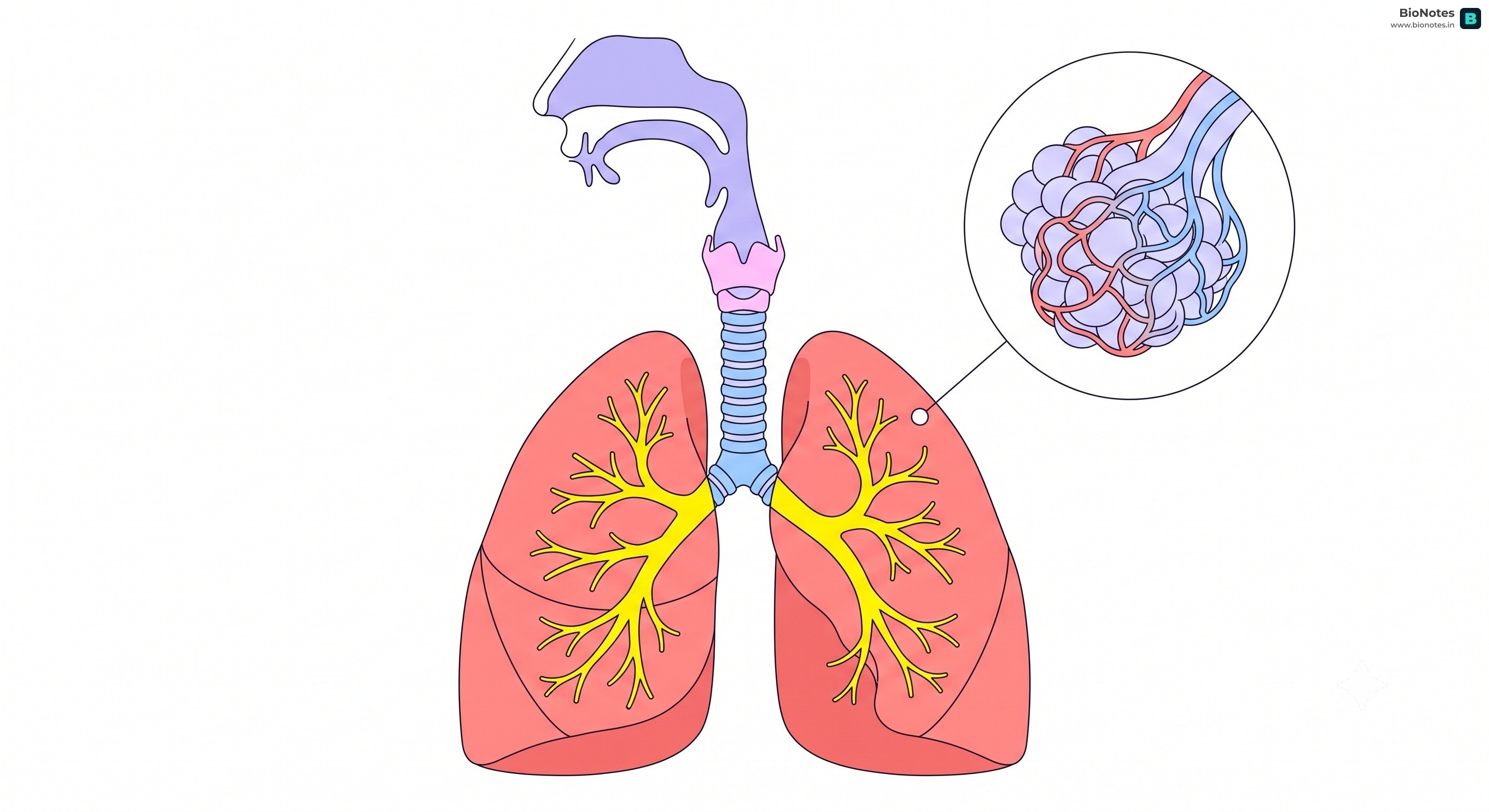
Note on Breathing and Exchange of Gases
Breathing involves two stages: inspiration (inhalation) and expiration (exhalation).
It is an active process.
The diaphragm contracts and flattens.
The external intercostal muscles contract, lifting the ribs and sternum upwards and outwards.
This increases the volume of the thoracic cavity, which in turn increases the volume of the lungs.
The pressure inside the lungs (intra-pulmonary pressure) decreases to less than the atmospheric pressure.
Air rushes from outside into the lungs.
Expiration (Exhalation):
Suction, not Pushing Humans use a negative pressure breathing system. We don't "push" air in; we expand our chest cavity to create a vacuum (lower pressure), and the outside air is "sucked" in to fill the space.
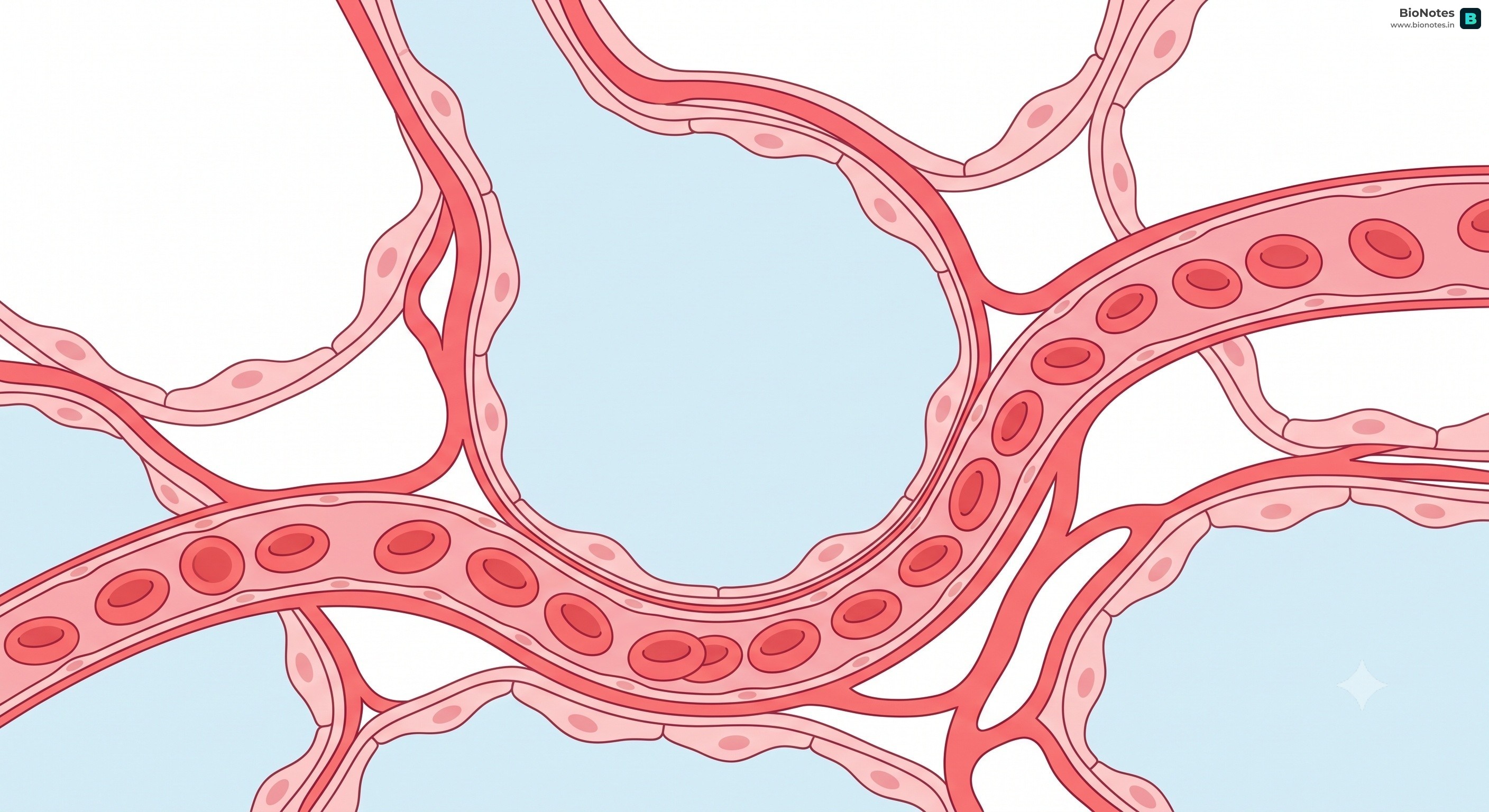
Gas exchange occurs in the alveoli and the tissues. It is a passive process of diffusion based on pressure/concentration gradients.
Alveolar Gas Exchange:
Tissue Gas Exchange:
Dissolved in Plasma: About 3% of O2 is transported in a dissolved state through blood plasma.
As Oxyhaemoglobin: About 97% of O2 is transported by red blood cells (RBCs). Oxygen binds with haemoglobin (a red-coloured iron-containing protein) in a reversible manner to form oxyhaemoglobin.
Hb + 4O2 ↔ Hb(O2)4Oxyhaemoglobin Dissociation Curve:
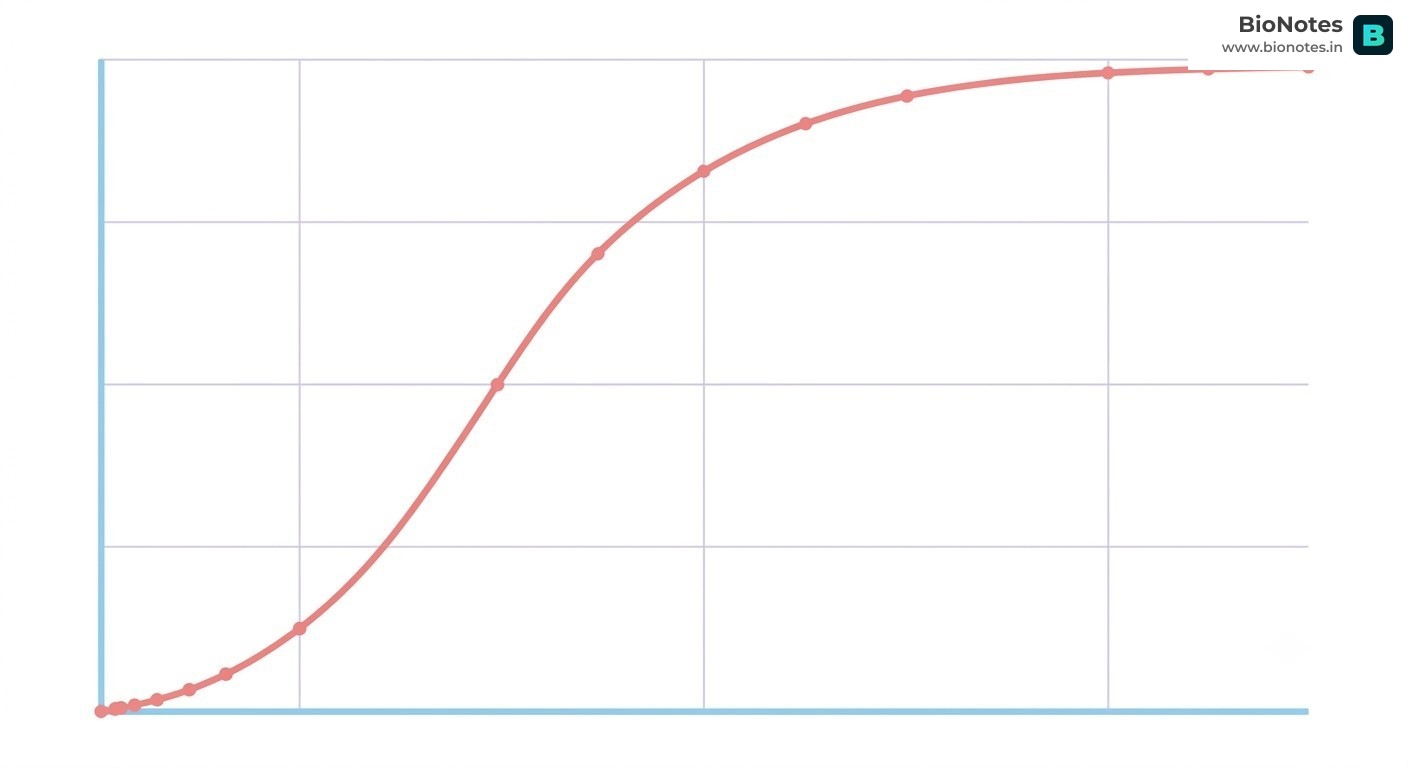
Competitive Edge: Bohr vs. Haldane Effect Don't mix these two up! They are two sides of the same coin:
As Bicarbonate Ions: About 70% of is transported as bicarbonate ions ().
Chloride Shift (Hamburger's Phenomenon):