Class 11
Created by Titas Mallick
Biology Teacher • M.Sc. Botany • B.Ed. • CTET (CBSE) • CISCE Examiner
Created by Titas Mallick
Biology Teacher • M.Sc. Botany • B.Ed. • CTET (CBSE) • CISCE Examiner
Online
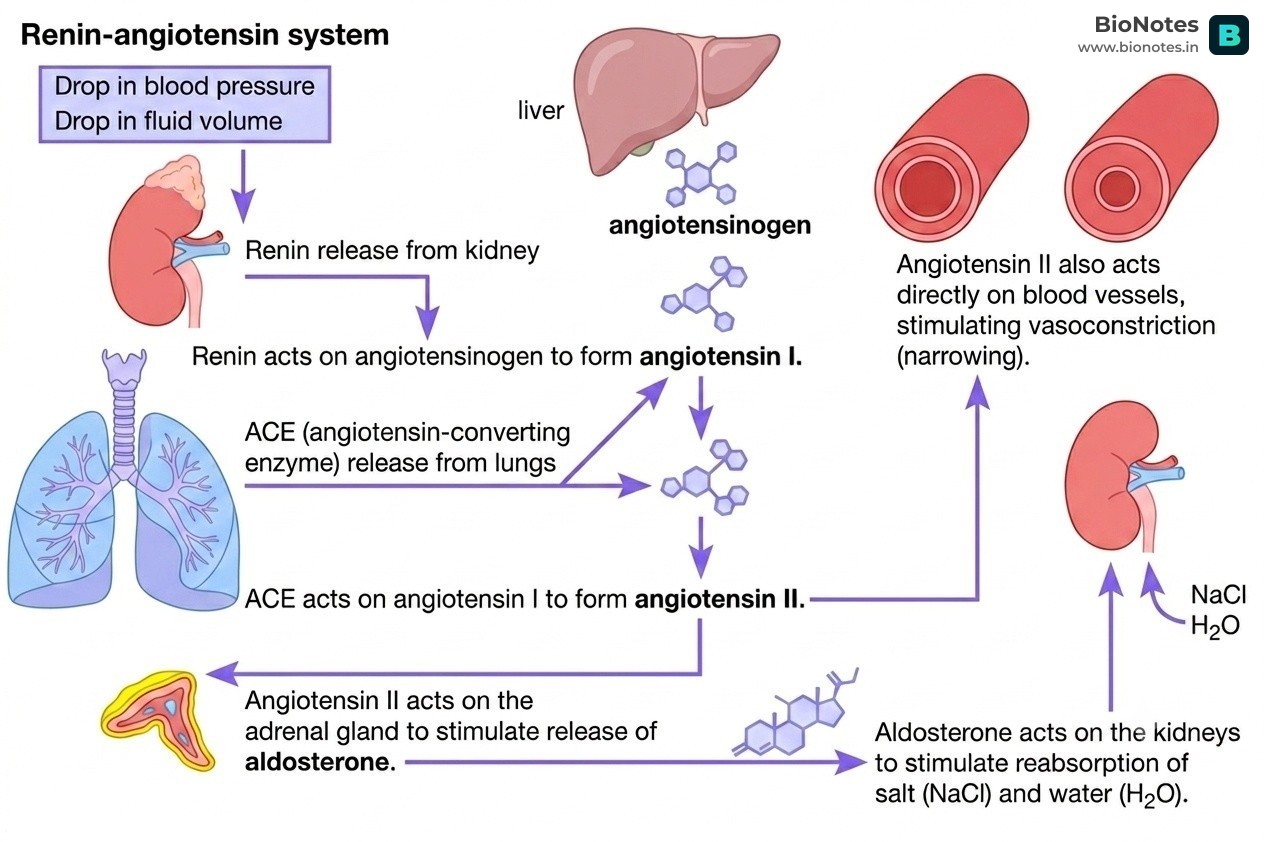
The Renin-Angiotensin-Aldosterone System (RAAS) is a complex, multi-organ endocrine cascade that is fundamental to the long-term regulation of arterial blood pressure, fluid volume, and sodium balance in the body. It is a critical homeostatic mechanism that ensures adequate tissue perfusion. Dysregulation of this system is a hallmark of many cardiovascular and renal diseases, including hypertension, heart failure, and chronic kidney disease, making it a primary target for pharmacological intervention.
| Component | Type | Source | Primary Function |
|---|---|---|---|
| Angiotensinogen | Pro-hormone (Zymogen) | Liver (primarily) | The inactive precursor substrate for the entire cascade. |
| Renin | Enzyme (Aspartate Protease) | Kidneys (Juxtaglomerular Cells) | Catalyzes the conversion of Angiotensinogen to Angiotensin I. |
| Angiotensin I | Peptide Hormone (Decapeptide) | Formed in circulation | A weak, largely inactive intermediate. |
| ACE | Enzyme (Dipeptidyl Carboxypeptidase) | Lungs (Vascular Endothelium) | Catalyzes the conversion of Angiotensin I to Angiotensin II. |
| Angiotensin II | Peptide Hormone (Octapeptide) | Formed in circulation | The main effector of the system. Potent vasoconstrictor and stimulator of Aldosterone and ADH release. |
| Aldosterone | Steroid Hormone | Adrenal Gland (Zona Glomerulosa) | Promotes sodium and water reabsorption in the kidneys. |
| ADH (Vasopressin) | Peptide Hormone | Posterior Pituitary | Promotes water reabsorption in the kidneys. |
The RAAS pathway is initiated in response to specific physiological signals indicating low blood pressure or fluid volume.
[STIMULUS]
│
┌──────────────────────────────────┴──────────────────────────────────┐
│ 1. Low Blood Pressure (Hypotension) detected by baroreceptors │
│ 2. Low Sodium Chloride ($NaCl$) concentration in distal tubule │
│ (detected by Macula Densa cells) │
│ 3. Sympathetic Nervous System stimulation (β1-adrenergic receptors) │
└──────────────────────────────────┬──────────────────────────────────┘
│
▼
[KIDNEY]
(Juxtaglomerular Apparatus)
│
└───── releases ─────▶ RENIN
│
│ (acts on)
▼
[LIVER] produces ───▶ ANGIOTENSINOGEN (circulating in blood) ◀───┘
│
│ (converted by Renin)
▼
ANGIOTENSIN I (Decapeptide, weak activity)
│
│ (travels via blood to the lungs)
▼
[LUNGS] produce ───▶ ANGIOTENSIN-CONVERTING ENZYME (ACE) ◀────┐
│ │ (also degrades Bradykinin)
│ (converted by ACE)
▼
**ANGIOTENSIN II (Octapeptide, POTENT)**
│
┌───────────────────┴───────────────────┐
│ │
▼ ▼
[EFFECTS] [FEEDBACK]
(See Section IV) (See Section V)Angiotensin II is the central actor in the RAAS pathway, exerting its effects by binding primarily to Angiotensin II Type 1 (AT1) receptors located on various target tissues.
Blood Pressure Target Because Angiotensin II is such a powerful vasoconstrictor, drugs that block its production (ACE Inhibitors) are among the most common treatments for high blood pressure.
While Angiotensin II provides the immediate pressor effect, Aldosterone and ADH are responsible for the longer-term volume restoration.
Key Distinction: Aldosterone reclaims both salt and water. ADH reclaims only water.
The ability of ADH to promote significant water reabsorption from the collecting duct is entirely dependent on the hypertonic interstitial fluid of the renal medulla. This steep osmotic gradient, increasing from the cortex (isotonic, ~300 mOsm/L) to the deep medulla (~1200 mOsm/L), is established and maintained by the counter-current mechanism. This mechanism involves two key components: the Loop of Henle and the Vasa Recta.
The Loop of Henle actively multiplies the concentration of the medullary interstitium.
Descending Limb:
Ascending Limb:
The "Multiplier" Effect: The key is that the salt pumped out by the ascending limb makes the interstitium salty, which in turn draws water out of the descending limb, concentrating the fluid that will then enter the ascending limb. This positive feedback loop creates the powerful osmotic gradient.
The Vasa Recta are the long, hairpin-shaped blood vessels that surround the Loop of Henle. Their job is to supply the medulla with blood without washing out the precious salt gradient created by the Loop of Henle.
The "Exchanger" Effect: The vasa recta acts as a passive exchanger. It removes the reabsorbed water but leaves the salt behind, thus preserving the medullary gradient that is essential for the final step of urine concentration.
The RAAS pathway culminates in the release of ADH. ADH makes the collecting duct permeable to water. Because the collecting duct passes through the hypertonic medulla created by the counter-current mechanism, there is a powerful osmotic force pulling water out of the filtrate and back into the body.
Without the counter-current mechanism, ADH would be useless, as there would be no osmotic gradient to drive water reabsorption. This is how the kidney, under the direction of RAAS, can produce a small volume of highly concentrated urine to conserve water and increase blood volume and pressure.
The RAAS pathway is tightly regulated to prevent dangerous hypertension.
As detailed in the flowchart, the system is turned ON by:
[HIGH BLOOD PRESSURE / HIGH BLOOD VOLUME]
│
┌───────────────────┴───────────────────┐
│ │
▼ ▼
[KIDNEY] [HEART (Atria)]
│ │
│ (Increased stretch/pressure │ (Stretched by high volume)
│ and high $NaCl$ at macula densa) │
│ │
└─▶ Inhibits RENIN Release └─▶ Releases ATRIAL NATRIURETIC PEPTIDE (ANP)
│
┌─────────────────────────┴─────────────────────────┐
│ │ │
▼ ▼ ▼
[Vasodilation] [Inhibits RENIN release] [Inhibits ALDOSTERONE release]
│ │ │
└───────────┬─────────────┘ │
│ │
▼ ▼
[DECREASES ANGIOTENSIN II] [Promotes $Na^+$ & Water Excretion]
│ │
└──────────────────┬────────────────────┘
│
▼
[LOWERED BLOOD PRESSURE]The central role of RAAS in hypertension makes it a prime target for medication.
| Drug Class | Examples | Mechanism of Action | Key Clinical Notes |
|---|---|---|---|
| ACE Inhibitors | Lisinopril, Ramipril, Enalapril | Block Angiotensin-Converting Enzyme (ACE), preventing the formation of Angiotensin II. | Side Effect: Dry Cough. ACE also breaks down bradykinin, a pro-inflammatory substance. Inhibiting ACE leads to bradykinin accumulation in the lungs, causing a cough. Also risk of angioedema. |
| ARBs | Losartan, Valsartan, Irbesartan | Angiotensin Receptor Blockers. Selectively block the AT1 receptor, preventing Angiotensin II from exerting its effects. | No cough. Because they do not affect ACE, bradykinin metabolism is normal. A good alternative for patients who cannot tolerate ACE inhibitors. |
| Direct Renin Inhibitors | Aliskiren | Binds directly to the active site of Renin, preventing it from converting angiotensinogen to angiotensin I. | Acts at the very top of the cascade. Less commonly used than ACEi/ARBs. |
| Aldosterone Antagonists | Spironolactone, Eplerenone | Block the mineralocorticoid receptor in the distal tubule/collecting duct, preventing aldosterone from working. | Also known as potassium-sparing diuretics. They promote and water excretion without causing loss. Spironolactone can cause gynecomastia; Eplerenone is more selective and has fewer side effects. |
The RAAS is a double-edged sword: essential for survival in acute situations (e.g., hemorrhage), but its chronic overactivation contributes to a wide range of cardiovascular and renal diseases.
In summary, understanding the RAAS pathway is crucial not only for comprehending fundamental cardiovascular and renal physiology but also for appreciating the rationale behind many life-saving medications used in clinical practice.
The body's ability to maintain blood pressure within a narrow, optimal range relies on the dynamic interplay between the RAAS (the pressure-raising system) and the ANP system (the pressure-lowering system).
| Feature | Renin-Angiotensin-Aldosterone System (RAAS) | Atrial Natriuretic Peptide (ANP) System |
|---|---|---|
| Primary Trigger | Low Blood Pressure, Low Blood Volume, Low , Sympathetic stimulation. | High Blood Pressure, High Blood Volume (atrial stretch). |
| Key Effector(s) | Angiotensin II, Aldosterone, ADH | Atrial Natriuretic Peptide (ANP) |
| Vascular Effect | Potent Vasoconstriction (raises systemic resistance). | Vasodilation (lowers systemic resistance). |
| Effect on Renal System | and Water Reabsorption (conserves volume). | and Water Excretion (natriuresis, diuresis). |
| Effect on GFR | Constricts efferent arteriole to maintain GFR. | Dilates afferent arteriole to increase GFR. |
| Effect on Renin | Is the result of renin release. | Inhibits renin release. |
| Effect on Aldosterone | Stimulates aldosterone release. | Inhibits aldosterone release. |
| End Result | INCREASES Blood Pressure & Blood Volume | DECREASES Blood Pressure & Blood Volume |
This constant "tug-of-war" ensures that blood pressure does not fall too low, compromising tissue perfusion, nor rise too high, damaging blood vessels and organs. When RAAS is activated and successfully raises blood pressure, that very increase in pressure and volume stretches the heart's atria, triggering the release of ANP to act as a brake, preventing overcorrection. This elegant feedback loop is central to cardiovascular homeostasis. ular homeostasis.