Class 11
Created by Titas Mallick
Biology Teacher • M.Sc. Botany • B.Ed. • CTET (CBSE) • CISCE Examiner
Created by Titas Mallick
Biology Teacher • M.Sc. Botany • B.Ed. • CTET (CBSE) • CISCE Examiner
Online
Movement is one of the significant features of living beings. It can be the movement of a part of the body or the whole organism. When a movement results in a change of place or location, it is called locomotion.
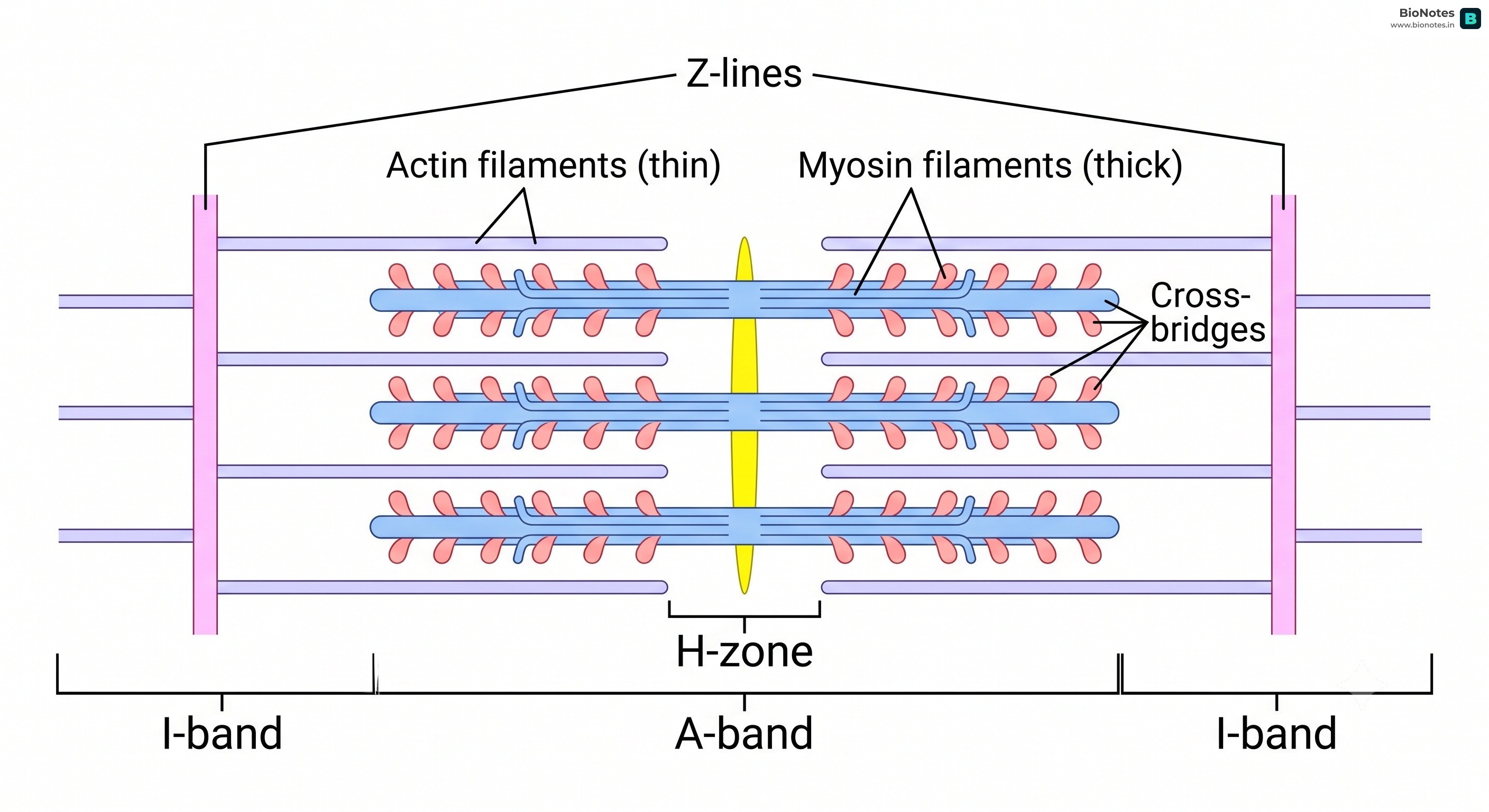
The Unit of Action The Sarcomere is the smallest functional unit of a muscle. When a muscle contracts, thousands of these tiny units shorten simultaneously, leading to the overall contraction of the muscle fiber.
ATP → ADP + Pi + Energy (This energy is used for the power stroke).Creatine Phosphate + ADP → Creatine + ATP (This reaction replenishes ATP).| Feature | Red Muscles (Slow Twitch) | White Muscles (Fast Twitch) |
|---|---|---|
| Myoglobin Content | High | Low |
| Mitochondria | Numerous | Few |
| Sarcoplasmic Reticulum | Less | More |
| Contraction Speed | Slow | Fast |
| Fatigue | Resistant | Prone to fatigue |
| Example | Extensor muscles of the back | Muscles of the eyeball |
Competitive Edge: The Sarcoplasmic Reticulum Trap A common misconception is that Red Muscles have "more of everything." While they do have more Myoglobin, Mitochondria, and blood capillaries, they actually have LESS Sarcoplasmic Reticulum compared to White Muscles! White muscles rely heavily on SR calcium release for fast, anaerobic bursts.
The human skeleton consists of 206 bones and is divided into the axial skeleton and the appendicular skeleton.
Joints are essential for all types of movements involving the bony parts of the body. They are points of contact between bones, or between bones and cartilages.