Class 11
Created by Titas Mallick
Biology Teacher • M.Sc. Botany • B.Ed. • CTET (CBSE) • CISCE Examiner
Created by Titas Mallick
Biology Teacher • M.Sc. Botany • B.Ed. • CTET (CBSE) • CISCE Examiner
Online
An Electrocardiogram (ECG or EKG) is a non-invasive diagnostic tool that records the electrical activity of the heart over a period of time. It detects the tiny electrical changes on the skin that arise from the heart muscle's electrophysiological pattern of depolarization and repolarization during each heartbeat. The ECG provides valuable information about the heart's rhythm, rate, and the condition of its conduction system and muscle.
To understand the ECG, it's crucial to grasp the basic electrical events within cardiac cells:
These cellular electrical events, when coordinated across millions of heart cells, generate electrical currents that can be detected on the body surface by electrodes.
The heart's electrical activity originates and propagates through a specialized conduction system:
SA Node (Pacemaker)
│
▼
Atrial Pathways
│
▼
AV Node (Delay)
│
▼
Bundle of His
│
┌─────────────────┴─────────────────┐
▼ ▼
Left Bundle Branch Right Bundle Branch
│ │
▼ ▼
Purkinje Fibers Purkinje Fibers
│ │
▼ ▼
Ventricular Myocardium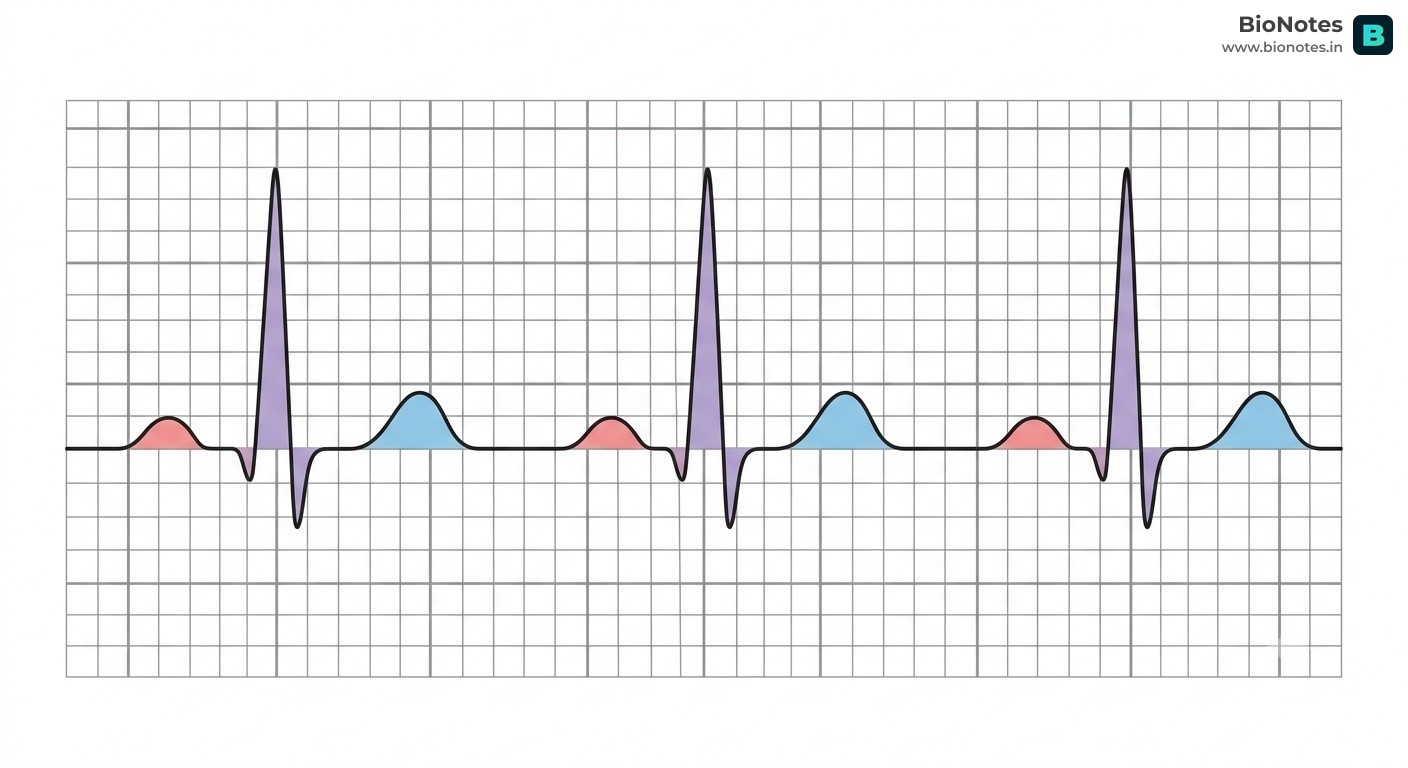
A typical ECG tracing consists of several waves, segments, and intervals, each representing a specific electrical event in the cardiac cycle.
R (Peak)
/ \
/ \
P (Atrial Depol.) / \ T (Ventricular Repol.)
/ \ / \ / \
/ \___________/ \_____________/ \___________
Q S
|--P--|--PR Seg--|----QRS----|--ST Seg--|------T------|
|---PR Interval---|
|-------------QT Interval------------|Size Matters The P-wave is small because the Atria have a relatively thin muscular wall compared to the Ventricles. A smaller muscle mass generates a smaller electrical signal.
QRS Complex:
T Wave:
U Wave (Optional):
PR Segment:
ST Segment:
PR Interval:
QT Interval:
Changes in the ECG waveforms, segments, and intervals can indicate various cardiac abnormalities, often linked to specific diseases or physiological changes.
| Anomaly | Description | Associated Condition(s) | Why the Change Occurs |
|---|---|---|---|
| Tall/Peaked P Wave | P wave > 2.5 mm in height. | Right Atrial Enlargement (e.g., Pulmonary Hypertension, Tricuspid Stenosis) | Increased pressure or volume in the right atrium causes its muscle to hypertrophy, generating a larger electrical signal. |
| Notched/Wide P Wave | P wave > 0.12 seconds in duration, often bifid. | Left Atrial Enlargement (e.g., Mitral Stenosis, Aortic Stenosis) | Delayed conduction through an enlarged left atrium, causing the two atrial depolarizations to be separated. |
| Absent P Wave | No visible P wave. | Atrial Fibrillation, Junctional Rhythm, Sinus Arrest | In AFib, chaotic atrial activity replaces organized depolarization. In junctional rhythm, the impulse originates in the AV node, bypassing the atria or causing retrograde atrial depolarization. |
| Inverted P Wave | P wave is negative in leads where it should be positive (e.g., Lead II). | Junctional Rhythm, Ectopic Atrial Rhythm | Impulse originates in the AV node or a low atrial focus, causing retrograde (backward) depolarization of the atria. |
| Anomaly | Description | Associated Condition(s) | Why the Change Occurs |
|---|---|---|---|
| Prolonged PR Interval | PR interval > 0.20 seconds. | First-Degree AV Block | Delayed conduction through the AV node. The impulse takes longer than normal to pass from the atria to the ventricles, but every impulse still gets through. |
| Short PR Interval | PR interval < 0.12 seconds. | Wolff-Parkinson-White (WPW) Syndrome, Lown-Ganong-Levine (LGL) Syndrome | Presence of an accessory pathway (e.g., Bundle of Kent in WPW) that bypasses the AV node, leading to premature ventricular activation. |
| Anomaly | Description | Associated Condition(s) | Why the Change Occurs |
|---|---|---|---|
| Wide QRS Complex | QRS duration > 0.12 seconds. | Bundle Branch Block (BBB), Ventricular Tachycardia (VT), Hyperkalemia | BBB: Blockage in one of the bundle branches causes delayed and abnormal depolarization of one ventricle. VT: Impulse originates in the ventricles, leading to slow, abnormal spread of depolarization. Hyperkalemia: High potassium levels impair rapid sodium influx, slowing conduction. |
| Tall R Wave | Abnormally high R wave amplitude. | Ventricular Hypertrophy (e.g., Left Ventricular Hypertrophy due to Hypertension) | Increased ventricular muscle mass generates a larger electrical signal. |
| Pathological Q Wave | Q wave > 0.04 seconds duration OR > 1/3 the height of the R wave in the same lead. | Myocardial Infarction (MI) - Necrosis | Represents electrical silence from necrotic (dead) myocardial tissue. The ECG records electrical activity from the opposite, healthy wall, creating a deep, wide Q wave. |
| Anomaly | Description | Associated Condition(s) | Why the Change Occurs |
|---|---|---|---|
| ST Elevation | ST segment elevated > 1 mm (or 2 mm in V2-V3) above the isoelectric line. | Acute Myocardial Infarction (STEMI), Pericarditis, Early Repolarization | STEMI: Indicates transmural ischemia (full thickness heart muscle injury) due to complete coronary artery occlusion. The injured cells have altered resting potentials and repolarization, causing a current of injury. Pericarditis: Inflammation of the pericardium causes diffuse ST elevation. |
| ST Depression | ST segment depressed > 0.5 mm below the isoelectric line. | Myocardial Ischemia, Non-STEMI, Digitalis Effect, Subendocardial Infarction | Ischemia: Indicates subendocardial ischemia (inner layer heart muscle injury) due to insufficient blood flow. The affected cells repolarize abnormally. Digitalis: Affects ion channels, causing characteristic ST depression. |
| Anomaly | Description | Associated Condition(s) | Why the Change Occurs |
|---|---|---|---|
| Tall/Peaked T Wave | T wave is unusually tall and narrow. | Hyperkalemia, Early Myocardial Ischemia | Hyperkalemia: High potassium levels accelerate repolarization, leading to a rapid, peaked T wave. Ischemia: Early stages of ischemia can cause localized changes in repolarization. |
| Inverted T Wave | T wave is negative in leads where it should be positive. | Myocardial Ischemia, Ventricular Hypertrophy, Bundle Branch Block | Ischemia: Delayed repolarization in ischemic areas causes the T wave to invert. Hypertrophy/BBB: Abnormal ventricular depolarization leads to abnormal repolarization. |
| Flattened T Wave | T wave has reduced amplitude. | Hypokalemia, Ischemia | Hypokalemia: Low potassium levels prolong repolarization, flattening the T wave. Ischemia: Can also cause flattened T waves. |
| Anomaly | Description | Associated Condition(s) | Why the Change Occurs |
|---|---|---|---|
| Prolonged QT Interval | QT interval is abnormally long (corrected QT, QTc > 0.44-0.46 seconds). | Congenital Long QT Syndrome, Electrolyte Imbalances (Hypokalemia, Hypomagnesemia, Hypocalcemia), Certain Medications (e.g., antiarrhythmics, some antibiotics, antipsychotics) | Delayed ventricular repolarization, increasing the risk of life-threatening ventricular arrhythmias like Torsades de Pointes. This is due to dysfunction of ion channels (often potassium channels) that are crucial for repolarization. |
| Short QT Interval | QT interval is abnormally short (QTc < 0.34 seconds). | Congenital Short QT Syndrome, Hypercalcemia, Digitalis Toxicity | Accelerated ventricular repolarization, also increasing arrhythmia risk. Due to accelerated ion channel activity (e.g., potassium channels) or altered calcium handling. |
The ECG is an indispensable tool in cardiology, offering a window into the heart's electrical health. By understanding the normal physiological basis of each wave and interval, and recognizing the deviations from normal, clinicians can diagnose a wide array of cardiac conditions, from subtle rhythm disturbances to acute myocardial infarctions. The changes observed on an ECG are direct manifestations of underlying cellular electrical events (depolarization and repolarization) and the structural or functional integrity of the heart's conduction system and muscle. This detailed understanding is critical for accurate diagnosis and appropriate patient management.